The Components of Each CYANOKIT
Each CYANOKIT consists of1: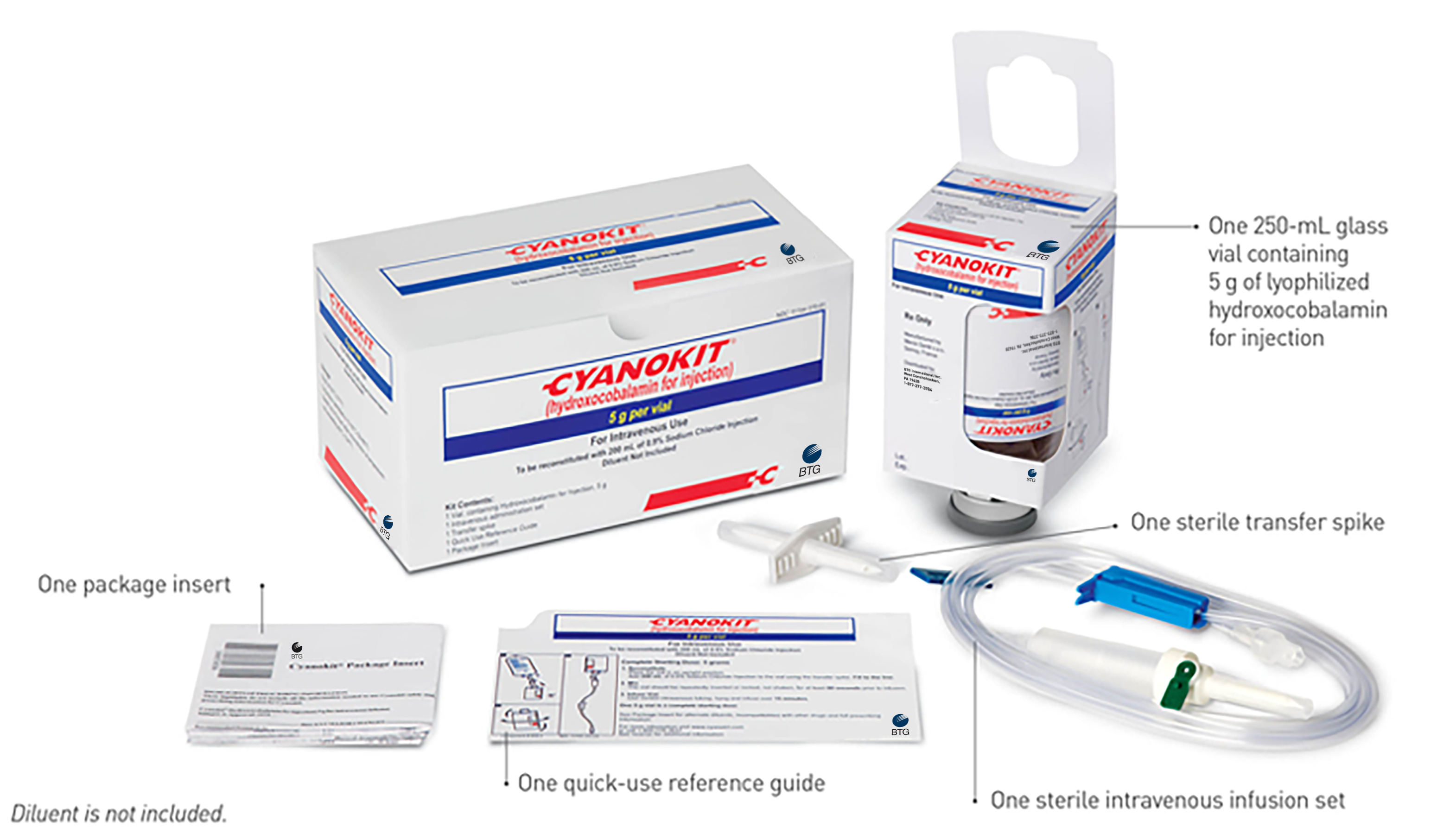
| NDC | Carton Dimensions |
|---|---|
NDC 50633-310-11 | W: 194 mm x L: 100 mm x H: 97 mm |
Dosing and Administration for CYANOKIT
Recommended Dosing for CYANOKIT1
- The starting dose of CYANOKIT for adults is 5 g (contained in a single vial), administered by IV infusion over 15 minutes (approximately 15 mL/min)*
- Depending upon the severity of the poisoning and the clinical response, a second dose of 5 g may be administered by IV infusion up to a total dose of 10 g
- The rate of infusion for a potential second dose may range from 15 minutes (for patients in extremis) to 2 hours, as clinically indicated
*No safety and efficacy studies have been performed in pediatric patients.
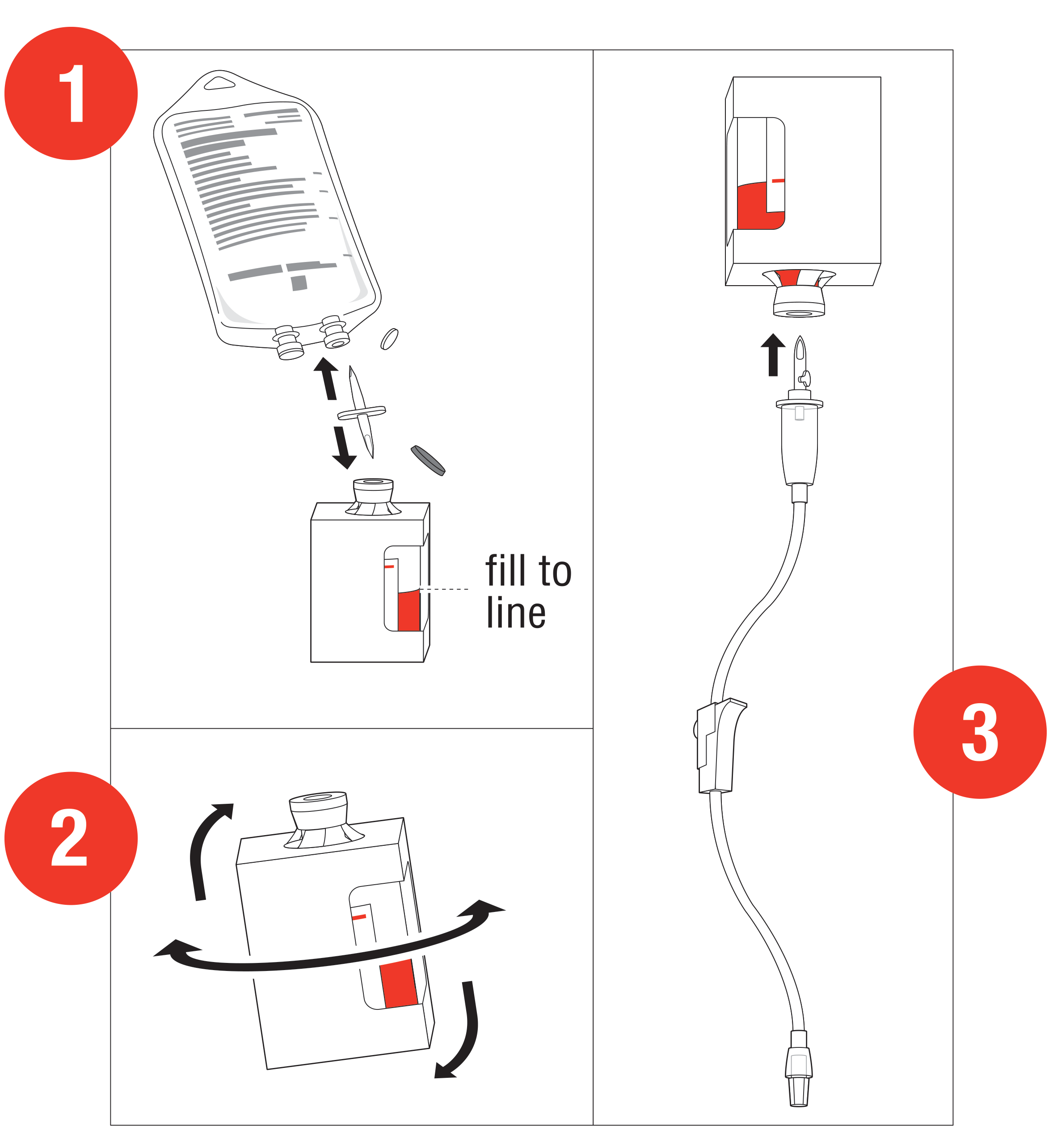
Preparation and Administration1
Starting dose: 5 g
- Reconstitute: Place the vial in an
upright position. Add 200 mL of 0.9% Sodium
Chloride injection† to the vial using the transfer
spike. Fill to the line.
†0.9% Sodium Chloride injection is the recommended diluent (diluent not included in the kit). Lactated Ringers injection and 5% Dextrose injection have also been found to be compatible with hydroxocobalamin and may be used if 0.9% Sodium Chloride is not readily available. - Mix: The
vial should be repeatedly inverted or rocked, not shaken, for at
least 60 seconds prior to infusion.
• CYANOKIT solutions should be visually inspected for particulate matter and color prior to administration
• Discard solution if particulate matter is present or solution is not dark red Infuse Vial: Use vented intravenous tubing, hang and infuse over 15 minutes.
The safety of administering other cyanide antidotes simultaneously with CYANOKIT has not been established. If a decision is made to administer another cyanide antidote with CYANOKIT, these drugs should not be administered concurrently in the same intravenous line.
CYANOKIT Incompatibility Information1
Physical incompatibility (particle formation) and chemical incompatibility were observed with the mixture of hydroxocobalamin in solution with select drugs that are frequently used in resuscitation efforts. Hydroxocobalamin is also chemically incompatible with sodium thiosulfate and sodium nitrite and has been reported to be incompatible with ascorbic acid. Therefore, these and other drugs should not be administered simultaneously through the same intravenous line as hydroxocobalamin.
Simultaneous administration of hydroxocobalamin and blood products (whole blood, packed red cells, platelet concentrate and/or fresh frozen plasma) through the same intravenous line is not recommended. However, blood products and hydroxocobalamin can be administered simultaneously using separate intravenous lines (preferably on contralateral extremities, if peripheral lines are being used).